The Workflow Everyone Hates
A medical director at a regional health plan described prior authorization to me as "the workflow nobody likes that everyone needs." Providers hate the administrative burden. Patients hate the delays. Plans hate the operational cost. The process exists for legitimate reasons (cost control, appropriate use review, fraud prevention) and produces friction at every step.
She told me her plan had been evaluating GenAI applications for prior authorization since 2023. By 2025, specific patterns had emerged that produced measurable improvement. Other patterns had been tried and abandoned because they produced regulatory exposure that outweighed the operational benefits.
The pattern of successful GenAI adoption in prior authorization is more constrained than the pattern in customer service or general productivity. The constraints come from the regulatory framework around utilization management. Knowing the constraints upfront produces applications that ship. Ignoring them produces applications that get pulled before reaching production.
Your AI Products Aren’t Stuck Because of Models
They’re stuck because the data layer they need doesn’t exist yet
Three Patterns That Produce Results
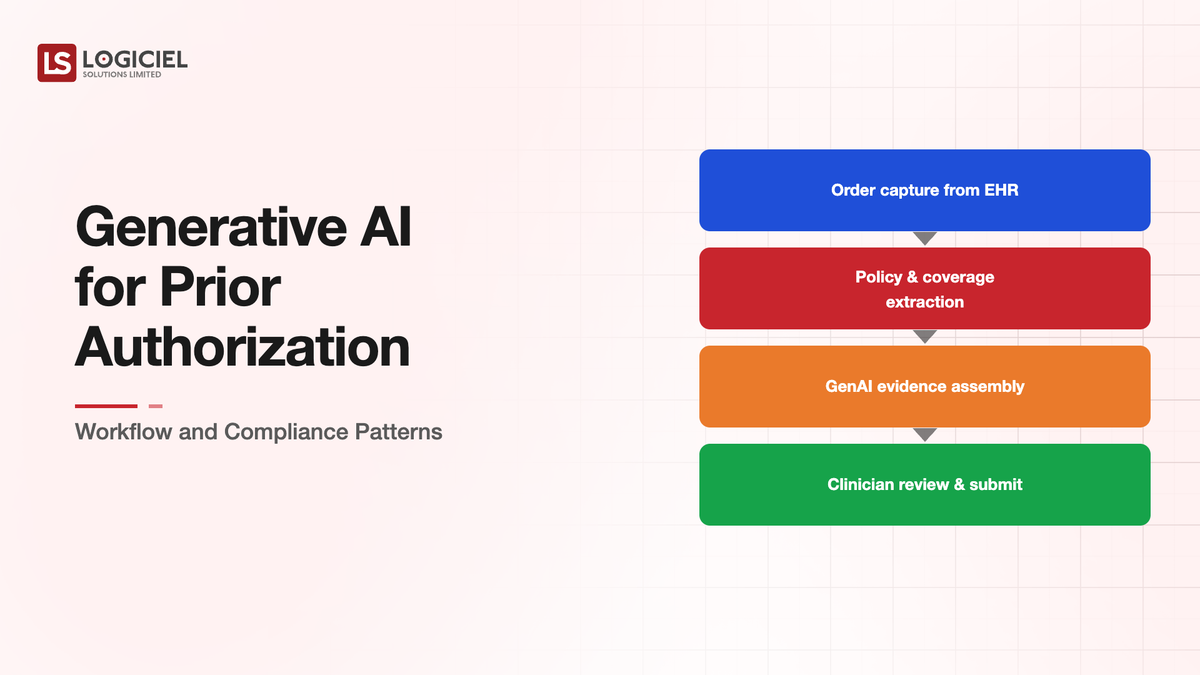
GenAI applications in prior authorization that have produced sustained results in 2024 and 2025 cluster around three workflow patterns.
The first pattern is intake automation and information extraction. Prior authorization requests arrive in many formats from many sources. Fax forms still dominate in some regions. Electronic submissions vary in structure. The intake step historically required substantial manual data entry to convert provider submissions into the plan's processing format.
GenAI handles this conversion with appropriate accuracy. The intake automation extracts clinical information, member identification, requested service codes, supporting documentation indicators, and other elements that the prior authorization workflow needs. The output goes into the plan's processing systems.
The pattern works because the intake step is information extraction rather than clinical decision-making. The AI is reading and structuring data, not deciding whether to approve. The regulatory framework treats this as administrative work rather than as clinical decisions.
The second pattern is provider communication and documentation request management. Many prior authorization decisions require additional documentation from providers. The plan requests specific documentation; the provider submits; the plan reviews. The communication cycle traditionally takes days and involves substantial manual coordination.
GenAI handles the communication layer. Generating documentation requests in clear language. Tracking provider responses. Surfacing incomplete submissions to clinical reviewers. Routing complete submissions back to the review workflow. The AI does not decide clinical questions; it manages the communication that supports clinical reviewers.
The third pattern is policy reference and decision support for clinical reviewers. Prior authorization decisions involve checking clinical policies, clinical guidelines, member benefits, and supporting evidence. The reviewers do this work manually historically. GenAI can surface relevant policy sections, summarize clinical evidence, and suggest the policy criteria that apply to a specific request.
The pattern produces value when the AI augments rather than replaces clinical decision-making. The clinical reviewer makes the decision. The AI surfaces information that the reviewer evaluates. The decision-making remains human; the information access becomes faster.
Three Patterns That Produce Regulatory Exposure
Three patterns have been tried and largely abandoned because they produce regulatory exposure that outweighs operational benefits.
The first pattern is autonomous clinical decision-making. The AI evaluates the prior authorization request against criteria and produces an approval or denial decision without clinical reviewer involvement. Some plans tried this for routine cases.
The pattern produces regulatory exposure because prior authorization decisions affect access to care. State and federal regulations around utilization management increasingly require human clinical involvement in adverse decisions. Class action lawsuits in 2023 and 2024 against plans that used autonomous AI denials accelerated the regulatory pressure.
Plans that have tried autonomous decisions have largely walked them back. The architectural pattern that works is AI-assisted human decisions rather than AI-autonomous decisions.
The second pattern is AI-generated clinical justifications without traceability. The AI generates the clinical reasoning that supports an approval or denial. The reasoning sounds plausible but cannot always be traced back to specific evidence or policy.
The pattern produces regulatory exposure because plans have to be able to justify their decisions during appeals and external review. AI-generated reasoning that cannot be defended in adversarial review is worse than no reasoning at all.
The architectural pattern that works is AI surfacing of supporting evidence with clinical reviewers writing or approving the justifications. The traceability stays intact. The AI accelerates the writing.
The third pattern is AI-driven utilization steering without disclosure. The AI suggests alternative treatments, providers, or service levels that produce different cost outcomes. The suggestions get incorporated into provider communications without clear identification.
The pattern produces regulatory exposure because utilization steering without member knowledge raises consumer protection concerns. Several states have introduced or are considering regulations specifically addressing AI-driven steering.
The architectural pattern that works is transparent AI assistance with clear disclosure to members about AI involvement. The transparency requirement is increasing across regulatory frameworks.
The Compliance Architecture That Supports the Workflow
GenAI applications in prior authorization that survive regulatory scrutiny share architectural characteristics.
Human review at decision points. The AI assists but does not decide. Clinical reviewers make approval and denial decisions. AI involvement is documented but not determining.
Audit trails sufficient for adversarial review. Every AI-assisted action is logged with full context. The logs support reconstruction during member appeals or regulatory examinations.
Disclosure to providers and members about AI involvement. The communications make clear when AI is involved in the workflow. The transparency satisfies the increasingly explicit regulatory expectations.
Bias monitoring across patient subpopulations. The AI's performance gets measured across demographic groups. Disparities trigger investigation and remediation. Bias monitoring is operational, not theoretical.
Calibration with state-specific regulatory requirements. The AI workflow accounts for varying state regulations around prior authorization timing, appeal rights, and disclosure. The system is configurable per state rather than applying one set of rules everywhere.
These architectural characteristics are not optional for serious production deployment. Applications that lack them face operational risk that grows over time as regulatory frameworks tighten.
What This Looks Like at Scale
A regional health plan operating GenAI for prior authorization in 2025 typically processes a few thousand to tens of thousands of authorizations per day across the workflows. The AI handles intake automation for nearly all requests, communication management for most, and decision support for the subset routed to clinical reviewers.
Operational metrics typically show 30-50 percent reduction in time to decision for routine requests, substantial reduction in time spent on documentation requests, and meaningful improvement in provider satisfaction with the prior authorization workflow.
The cost economics typically work. The AI infrastructure cost is modest relative to the operational cost savings. The implementation cost is meaningful but pays back within twelve to eighteen months for most plans.
The regulatory and reputational considerations are what gate adoption more than the operational economics. Plans that build the compliance architecture alongside the operational improvement ship and sustain the applications. Plans that focus on operational improvement and treat compliance as overhead struggle to maintain the applications in production.
Silent Lead Leakage
Discover how 1–8% of real estate leads disappear before reaching your CRM.
What Logiciel Does Here
Logiciel works with health plan technology teams and the partners that build prior authorization applications. The work is typically structured around workflow design that fits the three productive patterns combined with compliance architecture that addresses the regulatory framework.
The Healthcare AI Implementation framework covers the three risk tiers that inform prior authorization specifically. The HITL Architectures for Enterprise Agentic AI framework covers the human-in-the-loop design that prior authorization requires.
A 30-minute working session is enough to assess your current or proposed prior authorization AI application against the workflow and compliance patterns.
Frequently Asked Questions
How is this different from existing rules-based prior authorization automation?
Rules-based automation handles structured cases with deterministic rules. GenAI handles unstructured intake and clinical context that rules cannot easily address. The two work together rather than as alternatives. Modern prior authorization platforms increasingly combine both.
What about the CMS regulations on AI in prior authorization?
CMS has proposed and is finalizing regulations on AI use in Medicare Advantage prior authorization. The regulations emphasize human review of adverse decisions, transparency, and documentation requirements. Plans should design AI applications anticipating these regulatory directions.
How do I handle appeals for AI-assisted decisions?
Through standard appeal processes with documentation that clearly identifies AI involvement. The appeal review is a human clinical review independent of the initial decision. The AI does not participate in appeals as decision-maker.
What about predictive prior authorization where AI predicts approval likelihood?
Predictive applications are emerging and face their own regulatory considerations. Predictions that affect provider behavior or member outcomes need the same architectural patterns as decision support. Pure analytical use cases have different risk profiles than decision-affecting use cases.
How does this work for specialty pharmacy prior authorization?
Specialty pharmacy prior authorization has its own complexity due to drug-specific protocols and patient-specific clinical criteria. The same three productive patterns apply with specialty-specific clinical guideline references. The compliance considerations are similar. Sources: - CMS, "Coverage Criteria for Medicare Advantage Plans," 2024 - HHS Office for Civil Rights HIPAA Reference