When One Region Stops Being Enough
A VP of cloud architecture at an academic medical center expanding into a second state told me about her team's first multi-region project in 2024. The medical center had been operating cloud workloads in one region for years. The expansion brought new compliance requirements (different state data residency expectations), new latency requirements (clinicians in the new state needed responsive applications), and new resilience requirements (the larger geographic footprint made regional outages more visible to leadership).
Her team spent eighteen months building the second-region capability. The work surfaced issues the original single-region architecture had concealed. Data flows that worked locally produced latency issues across regions. Failover patterns that existed in theory had not been tested. Compliance documentation that satisfied one state did not satisfy the other.
The pattern is common as healthcare organizations grow geographically. Single-region cloud architectures hide complexities that multi-region architectures expose. Knowing the patterns that handle multi-region complexity reduces the surprise factor when the expansion happens.
Four patterns address most of the realistic multi-region complexity in healthcare cloud.
Why Best-Of-Breed Stacks Quietly Become a Tax
Inside a 7-month consolidation that cut six tools to one and saved $1.4M.
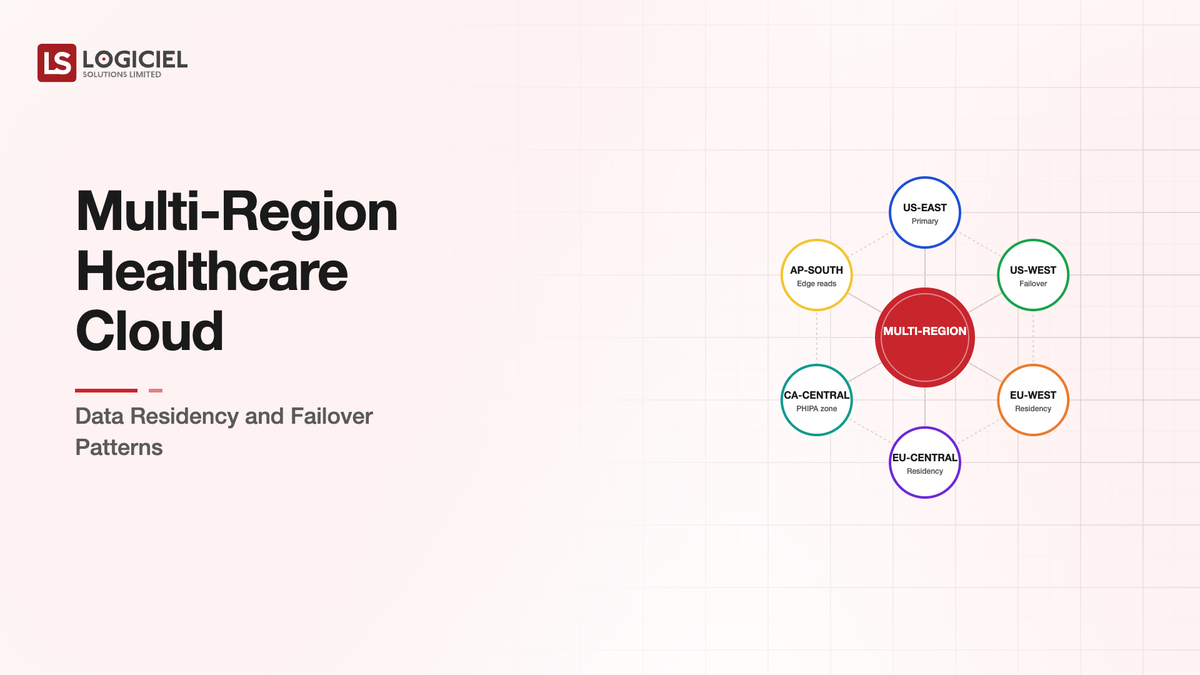
Pattern One: Data Residency Mapping by Workload
The first pattern is explicit mapping of which workloads have what data residency requirements.
Healthcare data residency requirements come from multiple sources. State laws vary in their specifics. Federal regulations apply uniformly. Patient-specific consent and provider-specific contractual obligations layer on top. The aggregate requirement for a specific workload may be specific.
The mapping exercise documents per-workload requirements. Patient data from State A patients lives in regions consistent with State A requirements. Patient data from State B patients lives in regions consistent with State B requirements. Operational data that does not include patient information may have more flexibility.
The mapping has to be granular enough to be enforceable in cloud configuration. Account-level segregation. VPC-level segregation. Bucket-level policies. The granularity matches the requirement granularity.
Organizations that do this mapping deliberately produce architectures that satisfy varied requirements. Organizations that operate without explicit mapping often discover compliance gaps when expansion or audit surfaces them.
Pattern Two: Multi-Region Architecture Per Application Type
The second pattern is per-application-type architecture decisions about how multi-region capability works.
Some applications are active in multiple regions simultaneously. Read and write traffic flows to the nearest region. Cross-region replication keeps regions consistent. The pattern fits applications where regional latency matters and where eventual consistency is acceptable for cross-region operations.
Some applications are active in one region with passive standby in another. Production traffic flows to the active region. The standby region maintains synchronized state and can become active in a regional outage. The pattern fits applications where strong consistency matters and where regional outages are the primary multi-region driver.
Some applications are partitioned by data residency. Patients from State A interact with the State A regional deployment. Patients from State B interact with the State B regional deployment. The applications run independently with shared management infrastructure. The pattern fits applications where data residency dominates over availability concerns.
The right pattern per application depends on the application's data residency, latency, consistency, and availability requirements. Most healthcare organizations end up with combinations across their application portfolio.
Pattern Three: Failover Design With Real Testing
The third pattern is failover design that has been tested under realistic conditions.
Failover that exists in theory often fails in practice when needed. The reasons are predictable. State that should have been replicated was not. Network paths that should have worked did not. DNS changes that should have propagated did not in the expected timeframe. Operational procedures that should have been clear were not.
The failover testing discipline that produces reliable failover includes regular scheduled tests, surprise tests that the operations team did not anticipate, partial failover tests that verify specific components, and full failover tests that exercise the complete process.
The tests produce findings. Each test finding gets addressed. The next test verifies the addressed finding. The compounding produces failover capability that actually works.
Organizations that document failover capability but do not test it have failover capability on paper. Organizations that test regularly have failover capability that works under stress.
The testing is uncomfortable. Real failover tests carry risk. Some organizations defer testing because of the risk and accept the alternative risk of untested failover when real incidents occur. The right balance is regular testing in controlled conditions with appropriate safety mechanisms.
Pattern Four: Cross-Region Data Flow Architecture
The fourth pattern is explicit architecture for data flows that span regions.
Some data has to move between regions for legitimate operational reasons. Population-level analytics need data from multiple regions. Cross-region patient transfers need data movement. Disaster recovery requires cross-region replication.
The architecture for these flows has to address residency requirements while enabling the operational need. The patterns include explicit aggregation services that produce de-identified data appropriate for cross-region movement, dedicated replication channels with appropriate encryption and access controls, and audit infrastructure that documents what data moved when and why.
Without explicit architecture, cross-region data flows happen ad-hoc. Engineering teams build pipelines that produce the operational result. Compliance teams discover the pipelines during audit. Remediation is more expensive than the upfront design.
The architecture decisions also affect operational complexity. Tightly controlled cross-region flows produce more compliance posture and more operational friction. Loosely controlled flows produce less compliance posture and easier operations. The balance is workload-specific.
What Goes Wrong With Multi-Region Healthcare Architecture
Three patterns of multi-region failure are common.
The first pattern is treating multi-region as a simple replication exercise. The team replicates resources across regions and assumes the architecture works. The reality is that multi-region introduces consistency, latency, and operational considerations that single-region architectures hide. The replication is necessary and not sufficient.
The second pattern is over-engineering the architecture before requirements are clear. The team builds elaborate multi-region capability assuming all workloads need it. The operational cost is high. Most workloads do not benefit from the capability proportionate to the cost.
The third pattern is under-investing in compliance documentation. The technical architecture supports multi-region. The compliance documentation does not address the multi-region specifics. Audits find documentation gaps that the architecture itself does not have.
Each pattern is preventable through deliberate planning. Per-workload requirements analysis. Per-workload architecture decisions. Compliance documentation that maps to the architecture decisions.
What This Costs
Multi-region healthcare cloud architecture costs meaningfully more than single-region. The premium comes from infrastructure duplication, cross-region data transfer, additional operational complexity, and increased compliance overhead.
The premium varies by pattern. Active-active multi-region is the most expensive. Active-passive is moderate. Partitioned by residency is variable depending on partition complexity. Cross-region disaster recovery is the least expensive option.
For organizations where multi-region is genuinely required, the cost is justified by the operational and compliance benefits. For organizations where multi-region is adopted without clear requirements, the cost can be substantial without proportionate benefit.
The decision about multi-region scope should follow workload-specific analysis rather than uniform application of multi-region patterns.
Why CFOs Reject Technical Cases And Approve Financial Ones
Inside a 5-step framework that won $500K of infrastructure budget in 14 days.
What Logiciel Does Here
Logiciel works with healthcare technology teams designing or operating multi-region cloud architectures. The work is typically structured around per-workload analysis, architecture pattern selection, and compliance documentation appropriate to the deployment scope.
The Cloud Architecture for Healthcare: HIPAA, HITRUST, and Real-time framework covers the broader healthcare cloud architecture decisions. The Disaster Recovery Architectures: RPO/RTO for AI Workloads framework covers the disaster recovery patterns that multi-region supports.
A 30-minute working session is enough to assess your current or proposed multi-region architecture against the four patterns.
Frequently Asked Questions
How do I decide which workloads need multi-region?
Through requirements analysis per workload. Data residency requirements. Latency requirements. Availability requirements. Workloads that have specific multi-region requirements benefit. Workloads without specific requirements usually do not justify the cost.
What about cross-cloud multi-region?
Different problem. Multi-cloud adds vendor diversity and complexity that multi-region within one cloud does not. The drivers for multi-cloud (vendor risk, capability differences) differ from the drivers for multi-region (residency, latency, availability). Most healthcare organizations operate multi-region within one cloud rather than full multi-cloud.
How does this work with state data residency variations?
Through explicit mapping. Each state's requirements get documented. The architecture enforces the requirements through configuration. The compliance documentation traces the architecture back to each state's specific requirements.
What is the right cadence for failover testing?
Quarterly full tests, monthly component tests, continuous monitoring of replication state. Less frequent testing produces failover capability that does not work under stress. More frequent testing has diminishing returns.
How does AI workload integration affect multi-region architecture?
AI workloads add cross-region considerations around model location, inference latency, and embedding storage. The multi-region architecture has to address AI workload patterns explicitly rather than assuming the general patterns cover AI cases. Sources: - AWS, "Multi-Region Architecture Best Practices," 2024 - HHS Office for Civil Rights HIPAA Reference