There is a payer-provider data exchange in your organization built point-to-point, custom-coded for each partner, predating the current interoperability rules. It works, sort of, but every new partner is a bespoke integration, every rule change means touching each connection, and the standards-based, API-driven exchange the new rules expect is bolted on at the edges rather than built in. The exchange was architected for a world of one-off integrations, and the rules have moved on.
This is more than legacy integration. It is payer-provider exchange architected for the old world facing new-world rules.
Payer-provider data exchange under the new rules is more than moving data between organizations. It is a standards-based, API-driven architecture, built on FHIR and the required exchange patterns, that supports the access, interoperability, and data-sharing the rules mandate, scales across many partners without bespoke integration, and stays compliant. The shift is from custom point-to-point to standards-based exchange.
However, many organizations bolt standards onto a point-to-point core and discover that the new rules expect an architecture, not a veneer.
If you are a healthcare technology leader at a payer or provider, the intent of this article is:
- Define what the new-rules payer-provider exchange requires
- Walk through standards-based, API-driven architecture
- Lay out the controls a compliant exchange needs
To do that, let's start with the basics.
Securing Multi-Tenant Healthcare AI When RBAC Isn't Enough
Why row-level security and application-layer RBAC are necessary but not sufficient for multi-tenant clinical AI.
What Is New-Rules Payer-Provider Exchange? The Basic Definition
At a high level, new-rules payer-provider data exchange is a standards-based, API-driven architecture, built on FHIR and mandated exchange patterns, that enables the data access and interoperability the rules require, scales across partners, and remains compliant.
To compare:
If point-to-point integration is building a separate private road to each partner, standards-based exchange is connecting to a shared highway system everyone uses. The roads must be rebuilt per partner; the highway scales to all of them and matches where the rules point.
Why Is New-Rules Exchange Architecture Necessary?
Issues that the architecture addresses or resolves:
- Meeting the access and interoperability the new rules mandate
- Scaling exchange across partners without bespoke integration
- Staying compliant as exchange requirements evolve
Resolved Issues by New-Rules Architecture
- Replaces point-to-point integration with standards-based exchange
- Supports the mandated APIs and data-sharing patterns
- Scales across partners and adapts to rule changes
Core Components of New-Rules Exchange
- Standards-based, API-driven exchange (FHIR)
- Support for mandated access and interoperability patterns
- Scalable connectivity across many partners
- Compliance and security controls
- Adaptability as rules evolve
Modern Payer-Provider Exchange Tooling
- FHIR APIs for standards-based exchange
- Implementation guides for the mandated patterns
- API gateways and partner connectivity
- Consent and access controls
- Audit and compliance tooling
These tools support new-rules exchange; the discipline is building standards-based architecture, not bolting standards onto point-to-point.
Other Core Issues They Will Solve
- Provide patient and partner data access as required
- Reduce the per-partner integration burden
- Give compliance evidence of standards-based exchange

Importance of New-Rules Exchange in 2026
Standards-based exchange matters more as interoperability rules tighten. Four reasons explain why it matters now.
1. The rules mandate standards-based access.
Current interoperability rules expect API-driven, standards-based exchange, FHIR and specified patterns, not custom point-to-point.
2. Point-to-point does not scale.
Bespoke integration per partner is unsustainable as the number of partners and the rule requirements grow.
3. Compliance is mandatory.
The exchange must meet regulatory requirements for access, interoperability, and privacy, not just move data.
4. Rules evolve.
Interoperability requirements change. A standards-based architecture adapts; a point-to-point one requires rework per change.
Traditional vs. New-Rules Exchange
- Point-to-point custom integration vs. standards-based API exchange
- Bespoke per partner vs. scalable shared patterns
- Standards bolted on vs. standards built in
- Rework per rule change vs. adaptable architecture
In summary: New-rules payer-provider exchange is standards-based and API-driven, scaling across partners and adapting to rules, not custom point-to-point.
Details About the Core Components of New-Rules Exchange: What Are You Designing?
Let's go through each layer.
1. Standards Layer
The basis of exchange.
Standards decisions:
- FHIR as the exchange standard
- Conformance to implementation guides
- Mandated patterns supported natively
2. API Layer
How data is exchanged.
API decisions:
- API-driven exchange, not file dumps
- The required access APIs implemented
- Standard interfaces for partners
3. Scalability Layer
How it grows.
Scalability decisions:
- Connectivity scaling across many partners
- Shared patterns over bespoke integration
- Onboarding new partners efficiently
4. Compliance Layer
How it meets the rules.
Compliance decisions:
- Access, interoperability, and privacy requirements met
- Consent honored in exchange
- Audit of data sharing
5. Adaptability Layer
How it handles change.
Adaptability decisions:
- Architecture that adapts as rules evolve
- Standards updates absorbed
- Minimal rework per change
Benefits Gained from Standards-Based Architecture
- The mandated access and interoperability supported
- Exchange that scales across partners without bespoke work
- Compliance maintained and adaptable as rules evolve
How It All Works Together
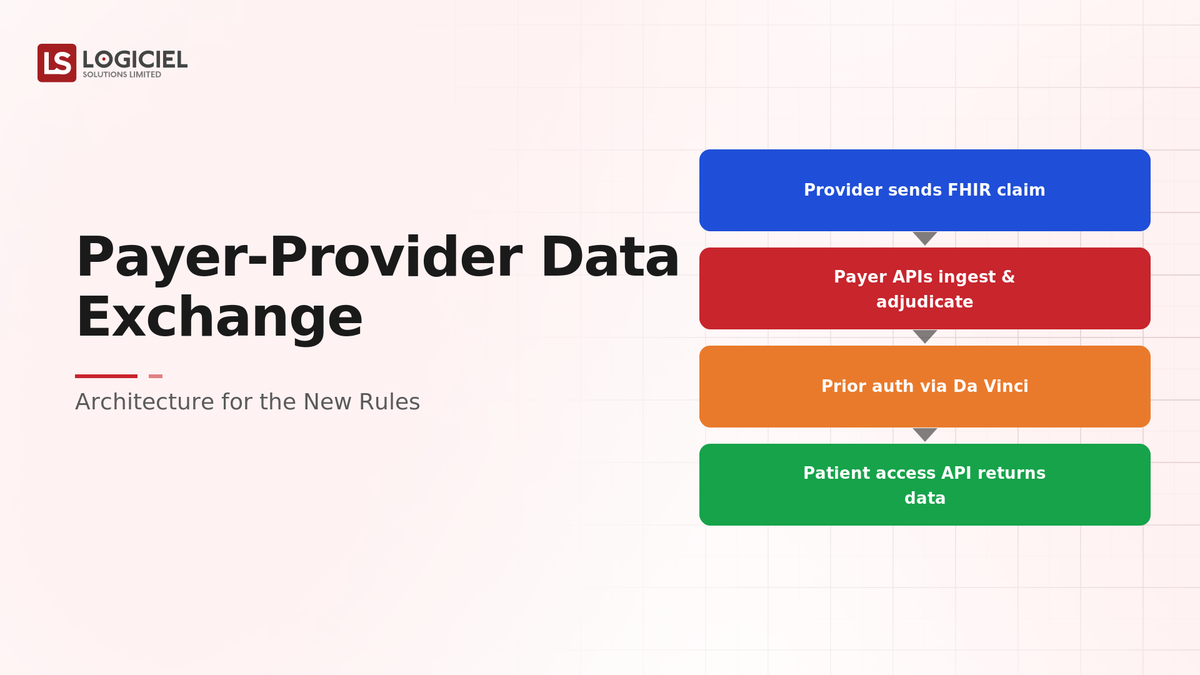
Exchange is built on FHIR and conforms to the mandated implementation guides, with the required access APIs implemented natively rather than as a veneer over a point-to-point core. Partners connect through standard interfaces, so onboarding a new partner uses shared patterns rather than bespoke integration, and the architecture scales across many of them. Consent is honored in exchange, access and privacy requirements are met, and data sharing is audited for compliance. As the rules evolve, the standards-based architecture absorbs updates with minimal rework. The exchange meets the new rules, scales, and adapts, rather than being a legacy point-to-point system with standards bolted on.
Common Misconception
Adding a FHIR API to our existing point-to-point exchange satisfies the new rules.
Bolting a FHIR API onto a point-to-point core is a veneer, not the standards-based architecture the rules expect. It does not scale across partners, does not natively support the mandated patterns, and requires rework per rule change. New-rules exchange requires standards built into the architecture, not added at the edge.
Key Takeaway: The new rules expect standards-based architecture, not a FHIR veneer over point-to-point. The difference is whether the exchange is standards-based or just speaks standards at the boundary.
Real-World New-Rules Exchange in Action
Let's take a look at how standards-based exchange operates with a real-world example.
We worked with an organization whose payer-provider exchange was point-to-point, with these constraints:
- Meet the new interoperability rules
- Scale across partners without bespoke integration
- Stay compliant and adaptable
Step 1: Adopt FHIR-Based Exchange
Build on the standard.
- FHIR as the exchange standard
- Conformance to implementation guides
- Mandated patterns supported
Step 2: Implement the Required APIs
Enable standards-based access.
- Required access APIs implemented
- Standard interfaces for partners
- API-driven, not file-based
Step 3: Scale Across Partners
Replace bespoke integration.
- Shared patterns over per-partner code
- Efficient partner onboarding
- Connectivity scaling
Step 4: Maintain Compliance
Meet the rules.
- Access, interoperability, privacy met
- Consent honored
- Data sharing audited
Step 5: Build for Adaptability
Handle rule changes.
- Architecture adapting to evolving rules
- Standards updates absorbed
- Minimal rework per change
Where It Works Well
- FHIR-based, API-driven exchange conforming to the patterns
- Scalable connectivity across partners via shared patterns
- Compliance maintained and architecture adaptable
Where It Does Not Work Well
- A FHIR veneer over point-to-point integration
- Bespoke integration per partner
- Rework per rule change
Key Takeaway: The exchange that meets the new rules is standards-based and API-driven, scaling across partners and adapting to rules, not point-to-point with standards bolted on.
Common Pitfalls
i) Bolting standards on point-to-point
A FHIR veneer over a point-to-point core does not scale or natively support the mandated patterns. Build standards into the architecture.
- Adopt FHIR as the model
- Implement required APIs natively
- Scale across partners
ii) Bespoke per-partner integration
Custom integration per partner is unsustainable. Use shared, standards-based patterns.
iii) Treating exchange as data movement only
The rules require access, interoperability, consent, and privacy, not just moving data. Meet the full requirements.
iv) Ignoring adaptability
Rules evolve. An architecture that requires rework per change is a liability. Build for adaptability.
Takeaway from these lessons: Most new-rules shortfalls trace to point-to-point cores with standards veneers, not to the standards. Build standards-based, scale across partners, and meet compliance.
New-Rules Exchange Best Practices: What High-Performing Teams Do Differently
1. Build standards into the architecture
Use FHIR and the mandated patterns as the architecture, not a veneer over point-to-point. The rules expect standards-based exchange.
2. Implement the required APIs natively
Support the mandated access APIs as part of the architecture, with standard interfaces for partners.
3. Scale across partners with shared patterns
Replace bespoke per-partner integration with shared, standards-based connectivity that onboards partners efficiently.
4. Meet the full compliance requirements
Access, interoperability, consent, and privacy, not just data movement. Audit data sharing.
5. Build for adaptability
Design so the architecture absorbs evolving rules with minimal rework, since interoperability requirements keep changing.
Logiciel's value add is helping payers and providers build standards-based, API-driven exchange on FHIR, scale across partners, and maintain compliance, so the architecture meets the new rules and adapts as they evolve.
Takeaway for High-Performing Teams: Focus on standards-based architecture, not a veneer. New-rules payer-provider exchange scales across partners and adapts to rules when standards are built in, while point-to-point with bolted-on standards does neither.
Signals You Are Architecting Exchange Correctly
How do you know the exchange meets the new rules? Not in whether you expose a FHIR API, but in whether the architecture is standards-based. Below are the signals that distinguish a real architecture from a veneer.
Exchange is standards-based. The team builds on FHIR and the mandated patterns as the architecture, not bolted on.
Partners onboard via shared patterns. New partners connect through standard interfaces, not bespoke integration.
Compliance requirements are met. Access, interoperability, consent, and privacy are satisfied and data sharing is audited.
The architecture scales. Exchange grows across many partners without per-partner custom code.
Rule changes are absorbed. The architecture adapts to evolving rules with minimal rework.
Adjacent Capabilities and Connected Work
This work does not exist in isolation. Payer-provider exchange depends on, and feeds into, several adjacent capabilities. Building one without thinking about the others is the most common scoping mistake.
In most health organizations, exchange shares infrastructure with the FHIR and data platform, the consent and access systems, and the compliance program. It shares capacity with integration engineering, IT, and the compliance teams. And it shares leadership attention with whatever the next interoperability initiative is on the roadmap. Naming these adjacencies upfront helps the program scope realistically and helps leadership see the work as a portfolio rather than a one-off project.
The most common mistake in adjacent-capability scoping is treating each adjacency as someone else's problem. The FHIR architecture the exchange depends on is your problem. The consent honored in exchange is your problem. The compliance audit of data sharing is your problem. Pretending otherwise pushes work to teams that did not plan for it, and the work returns to you later as a compliance gap or an unscalable integration. Own the adjacencies you depend on; partner with the teams that own them; share the timeline.
Conclusion
New-rules payer-provider data exchange is a standards-based, API-driven architecture that meets the mandated access and interoperability, scales across partners, and adapts to evolving rules. The discipline that delivers it is the same discipline behind any standards adoption: build on the standard, scale through shared patterns, and stay compliant.
Key Takeaways:
- The new rules expect standards-based architecture, not a FHIR veneer
- Build on FHIR and the mandated patterns, scaling across partners
- Meet the full compliance requirements and build for adaptability
Architecting new-rules exchange well requires standards, scalability, and compliance discipline. When done correctly, it produces:
- The mandated access and interoperability supported
- Exchange that scales across partners without bespoke work
- Compliance maintained and audited
- An architecture that adapts as the rules evolve
Where Health Data Standards Break in Real Systems
Why FHIR R4 certification does not equal FHIR interoperability, the specific data availability.
What Logiciel Does Here
If your payer-provider exchange is point-to-point with standards bolted on, rebuild it standards-based on FHIR, implement the required APIs natively, scale across partners, and build for adaptability.
Learn More Here:
- FHIR-Native Architectures: Designing for Interoperability
- Healthcare Interoperability Beyond FHIR: HL7v2, X12, and the Real Mix
- Consent Management for Healthcare AI: Patterns and Pitfalls
At Logiciel Solutions, we work with payer and provider technology leaders on standards-based data exchange, FHIR architecture, and interoperability compliance. Our reference patterns come from production healthcare exchange programs.
Explore how to architect payer-provider data exchange for the new rules.
Frequently Asked Questions
What do the new rules require for payer-provider data exchange?
Standards-based, API-driven exchange, built on FHIR and specified implementation guides and patterns, supporting mandated data access and interoperability, with consent and privacy honored. The expectation is an architecture, not custom point-to-point integration with standards added at the edge.
Isn't adding a FHIR API to our existing exchange enough?
No. Bolting a FHIR API onto a point-to-point core is a veneer that does not scale across partners, does not natively support the mandated patterns, and requires rework per rule change. The rules expect standards built into the architecture.
Why doesn't point-to-point integration work under the new rules?
Because bespoke integration per partner is unsustainable as partners and requirements grow, and it does not natively support the standards-based access the rules mandate. Standards-based exchange uses shared patterns that scale across partners and adapt to rule changes.
How do we make the exchange adaptable to evolving rules?
By building on standards, FHIR and the mandated patterns, as the architecture, so standards updates are absorbed with minimal rework. A point-to-point architecture requires custom rework per change, while a standards-based one adapts.
What is the biggest mistake in payer-provider exchange?
Bolting standards onto a point-to-point core and treating it as compliant. This veneer does not scale, does not natively support the mandated patterns, and breaks on rule changes. Build standards-based, API-driven architecture on FHIR, scale across partners, and meet the full compliance requirements.