There is an integration layer in your health system that translates everything into FHIR at the edge and immediately back out of FHIR internally, because the systems behind it speak their own proprietary models. FHIR is a thin veneer over an architecture that is not interoperable underneath. Every new partner means a new translation, every data model change ripples through mappings, and the promised interoperability stops at the integration boundary.
This is more than a translation layer. It is FHIR used as a gateway veneer rather than as the architecture.
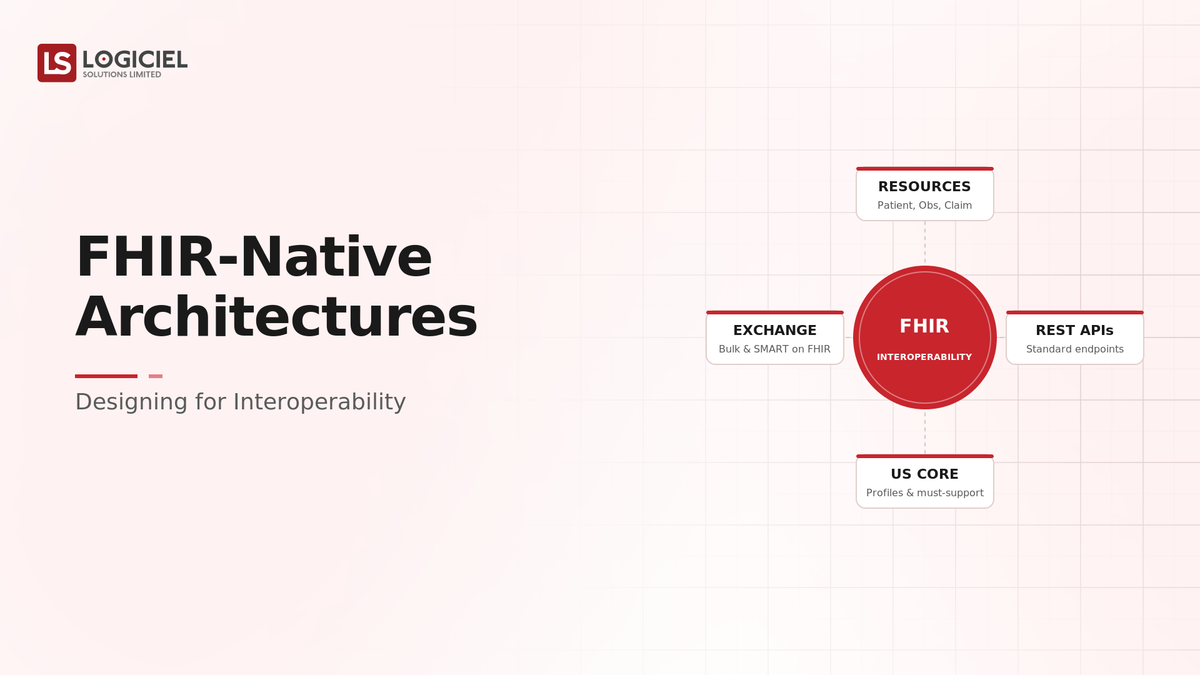
A FHIR-native architecture uses FHIR as the actual data model, not a format you translate to at the boundary. Resources are modeled in FHIR internally, stored and exchanged as FHIR, so interoperability is a property of the system rather than a translation bolted on at the edge. The difference is whether FHIR is what the system is, or just what it speaks to outsiders.
However, many teams adopt FHIR as an edge translation over a proprietary core and discover that veneer interoperability does not deliver the seamless exchange FHIR-native architecture does.
If you are a healthcare architect or technology leader, the intent of this article is:
- Define what FHIR-native means versus FHIR as a translation layer
- Walk through modeling, storing, and exchanging as FHIR
- Lay out the controls a FHIR-native architecture needs
To do that, let's start with the basics.
90-Day AI Production Guide for CTOs
Move AI from demo to durable production system, without burning your roadmap.
What Is a FHIR-Native Architecture? The Basic Definition
At a high level, a FHIR-native architecture uses FHIR resources as the internal data model, stored and exchanged as FHIR, so interoperability is built into the system rather than achieved by translating to FHIR at the boundary.
To compare:
If edge-translation FHIR is speaking a common language only when foreigners visit while thinking in your own at home, FHIR-native is thinking and operating in the common language throughout. The first requires constant translation and loses nuance; the second is genuinely interoperable.
Why Is FHIR-Native Architecture Necessary?
Issues that FHIR-native architecture addresses or resolves:
- Delivering real interoperability rather than edge-veneer translation
- Reducing the per-partner translation and mapping burden
- Making FHIR the model so exchange is seamless
Resolved Issues by FHIR-Native Architecture
- Replaces translation layers with native FHIR exchange
- Cuts the mapping burden of a proprietary core
- Makes interoperability a system property
Core Components of a FHIR-Native Architecture
- FHIR resources as the internal data model
- FHIR-native storage and APIs
- Standard FHIR exchange with partners
- Profiles and extensions for local needs
- Versioning and conformance management
Modern FHIR Tooling
- FHIR servers and data stores
- FHIR APIs following the standard
- Implementation guides and profiles
- Terminology services for coded data
- Conformance and validation tooling
These tools support FHIR-native architecture; the discipline is using FHIR as the model, not a gateway format.
Other Core Issues They Will Solve
- Enable seamless exchange with FHIR-based partners and platforms
- Support standards-based analytics and AI on healthcare data
- Reduce the cost of each new interoperability connection

Importance of FHIR-Native Architecture in 2026
FHIR-native design matters more as interoperability mandates and FHIR adoption grow. Four reasons explain why it matters now.
1. FHIR is the interoperability standard.
FHIR has become the standard for healthcare data exchange. Building native to it aligns with where the ecosystem is.
2. Edge translation does not scale.
A proprietary core with FHIR translation at the edge multiplies mapping work per partner and per change. Native FHIR removes that.
3. Interoperability is increasingly mandated.
Regulatory and market pressure toward interoperability rewards systems that are FHIR-native rather than superficially FHIR-compatible.
4. AI and analytics benefit from a standard model.
Standards-based data is easier to use across analytics and AI. A FHIR-native model provides that consistency.
Traditional vs. FHIR-Native Architecture
- FHIR translation at the edge vs. FHIR as the internal model
- Proprietary core vs. FHIR-native storage and APIs
- Per-partner mapping vs. standard FHIR exchange
- Veneer interoperability vs. interoperability as a system property
In summary: A FHIR-native architecture uses FHIR as the model throughout, making interoperability intrinsic rather than a boundary translation.
Details About the Core Components of a FHIR-Native Architecture: What Are You Designing?
Let's go through each layer.
1. Model Layer
How data is represented.
Model decisions:
- FHIR resources as the internal model
- Data thought of as FHIR, not translated to it
- Local concepts mapped to FHIR resources
2. Storage Layer
How data is stored.
Storage decisions:
- FHIR-native storage or a FHIR server
- Resources persisted as FHIR
- Querying via FHIR semantics
3. Exchange Layer
How data moves with partners.
Exchange decisions:
- Standard FHIR APIs for exchange
- Conformance to implementation guides
- Seamless interoperability with FHIR partners
4. Profile Layer
How local needs are met.
Profile decisions:
- Profiles and extensions for local requirements
- Extending FHIR within the standard
- Avoiding proprietary divergence
5. Conformance Layer
How quality is maintained.
Conformance decisions:
- Validation against FHIR specifications
- Versioning as FHIR and profiles evolve
- Terminology services for coded data
Benefits Gained from FHIR-Native Design
- Real interoperability as a system property, not a veneer
- Reduced per-partner mapping and translation burden
- Standards-based data ready for analytics and AI
How It All Works Together
Data is modeled as FHIR resources internally, not translated to FHIR at the boundary, with local concepts mapped to FHIR resources rather than to a proprietary model. It is stored in FHIR-native storage and queried with FHIR semantics, and exchanged with partners through standard FHIR APIs conforming to implementation guides, so interoperability is seamless rather than a translation. Profiles and extensions meet local needs within the standard, avoiding proprietary divergence. Validation, versioning, and terminology services maintain conformance as FHIR evolves. Interoperability becomes a property of the system, and each new connection costs far less than a bespoke mapping over a proprietary core.
Common Misconception
Supporting FHIR at our API boundary makes us interoperable.
Translating to FHIR at the edge over a proprietary core is veneer interoperability. It loses nuance in translation, multiplies mapping work per partner, and does not deliver the seamless exchange of a FHIR-native system. Real interoperability comes from using FHIR as the model, not just speaking it to outsiders.
Key Takeaway: There is a difference between speaking FHIR at the boundary and being FHIR-native. The former is a translation layer; the latter is interoperability built into the architecture.
Real-World FHIR-Native Architecture in Action
Let's take a look at how FHIR-native design operates with a real-world example.
We worked with a health system whose FHIR support was an edge translation over a proprietary core, with these constraints:
- Deliver real interoperability, not a veneer
- Reduce the per-partner mapping burden
- Use FHIR as the model
Step 1: Model in FHIR
Adopt FHIR resources as the internal model.
- Local concepts mapped to FHIR resources
- Data represented as FHIR internally
- Proprietary model retired where feasible
Step 2: Store Natively
Persist data as FHIR.
- FHIR-native storage or server
- Resources stored as FHIR
- FHIR query semantics
Step 3: Exchange via Standard FHIR
Connect with partners natively.
- Standard FHIR APIs
- Conformance to implementation guides
- Seamless partner exchange
Step 4: Profile for Local Needs
Meet requirements within the standard.
- Profiles and extensions for local needs
- Extending within FHIR
- Avoiding proprietary divergence
Step 5: Maintain Conformance
Keep quality as FHIR evolves.
- Validation against specifications
- Versioning as profiles change
- Terminology services for coded data
Where It Works Well
- FHIR as the internal model, stored and exchanged natively
- Standard FHIR exchange reducing per-partner mapping
- Profiles meeting local needs within the standard
Where It Does Not Work Well
- FHIR translation at the edge over a proprietary core
- Per-partner mappings that multiply with each connection
- Proprietary divergence that breaks conformance
Key Takeaway: The architecture that is genuinely interoperable is the one where FHIR is the model throughout, not the one that speaks FHIR at the boundary over a proprietary core.
Common Pitfalls
i) FHIR as an edge veneer
Translating to FHIR at the boundary over a proprietary core loses nuance and multiplies mapping. Use FHIR as the internal model.
- Model data as FHIR
- Store and exchange natively
- Avoid the translation core
ii) Per-partner mapping
A proprietary core forces bespoke mapping for each partner. Native FHIR exchange removes that burden.
iii) Proprietary divergence
Extending FHIR with proprietary, non-conformant changes breaks interoperability. Use profiles and extensions within the standard.
iv) Ignoring conformance
FHIR and profiles evolve. Without validation and versioning, conformance drifts. Maintain it actively.
Takeaway from these lessons: Most interoperability shortfalls trace to FHIR as a veneer and proprietary divergence, not to FHIR itself. Use FHIR as the model and stay conformant.
FHIR-Native Best Practices: What High-Performing Teams Do Differently
1. Use FHIR as the model, not a format
Model, store, and exchange data as FHIR internally, so interoperability is intrinsic rather than a boundary translation.
2. Avoid the proprietary core
A proprietary core with edge translation multiplies mapping and loses nuance. Native FHIR removes both problems.
3. Profile within the standard
Meet local needs with FHIR profiles and extensions rather than proprietary divergence that breaks conformance.
4. Maintain conformance actively
Validate against FHIR specifications, version as profiles evolve, and use terminology services for coded data.
5. Design for the ecosystem
Build native to where the interoperability ecosystem is, so each new FHIR partner connection is cheap rather than bespoke.
Logiciel's value add is helping health systems adopt FHIR as the internal model, store and exchange natively, profile within the standard, and maintain conformance, so interoperability is a system property rather than an edge veneer.
Takeaway for High-Performing Teams: Focus on using FHIR as the model throughout. The difference between speaking FHIR at the boundary and being FHIR-native is the difference between veneer and real interoperability.
Signals You Are FHIR-Native Correctly
How do you know the architecture is genuinely interoperable? Not in whether you expose a FHIR API, but in whether FHIR is the model. Below are the signals that distinguish FHIR-native from a veneer.
FHIR is the internal model. The team models, stores, and queries data as FHIR, not a proprietary model translated at the edge.
Exchange is standard FHIR. Partner connections use standard FHIR APIs conforming to implementation guides.
Per-partner mapping is minimal. New FHIR partner connections are cheap because the core is native, not mapped per partner.
Local needs use profiles. Local requirements are met with FHIR profiles and extensions within the standard.
Conformance is maintained. The team validates against specifications and versions as FHIR and profiles evolve.
Adjacent Capabilities and Connected Work
This work does not exist in isolation. A FHIR-native architecture depends on, and feeds into, several adjacent capabilities. Building one without thinking about the others is the most common scoping mistake.
In most health systems, FHIR-native design shares infrastructure with the EHR and source systems, the data platform, and the terminology and standards governance. It shares capacity with clinical informatics, data engineering, and the integration teams connecting partners. And it shares leadership attention with whatever the next interoperability initiative is on the roadmap. Naming these adjacencies upfront helps the program scope realistically and helps leadership see the work as a portfolio rather than a one-off project.
The most common mistake in adjacent-capability scoping is treating each adjacency as someone else's problem. The terminology services that code FHIR data are your problem. The source-system mapping to FHIR resources is your problem. The conformance validation is your problem. Pretending otherwise pushes work to teams that did not plan for it, and the work returns to you later as a broken integration. Own the adjacencies you depend on; partner with the teams that own them; share the timeline.
Conclusion
A FHIR-native architecture makes interoperability a property of the system by using FHIR as the model, not a translation at the edge. The discipline that delivers it is the same discipline behind any standards adoption: adopt the standard as the model, conform to it, and extend within it.
Key Takeaways:
- FHIR-native uses FHIR as the internal model, not a boundary format
- It delivers real interoperability and cuts per-partner mapping
- Profile within the standard and maintain conformance as FHIR evolves
Building FHIR-native well requires model, exchange, and conformance discipline. When done correctly, it produces:
- Real interoperability as a system property
- Reduced per-partner mapping and translation burden
- Standards-based data ready for analytics and AI
- Cheaper, seamless connections with FHIR partners
Safe LLM Integration Into Clinical Workflows
A clinical AI integration playbook for Chief Medical Officers responsible for clinician trust and patient safety.
What Logiciel Does Here
If your FHIR support is an edge veneer over a proprietary core, adopt FHIR as the internal model, store and exchange natively, profile within the standard, and maintain conformance.
Learn More Here:
- Healthcare Interoperability Beyond FHIR: HL7v2, X12, and the Real Mix
- Data Engineering for Healthcare: Unifying EHR, Claims, and Device Data
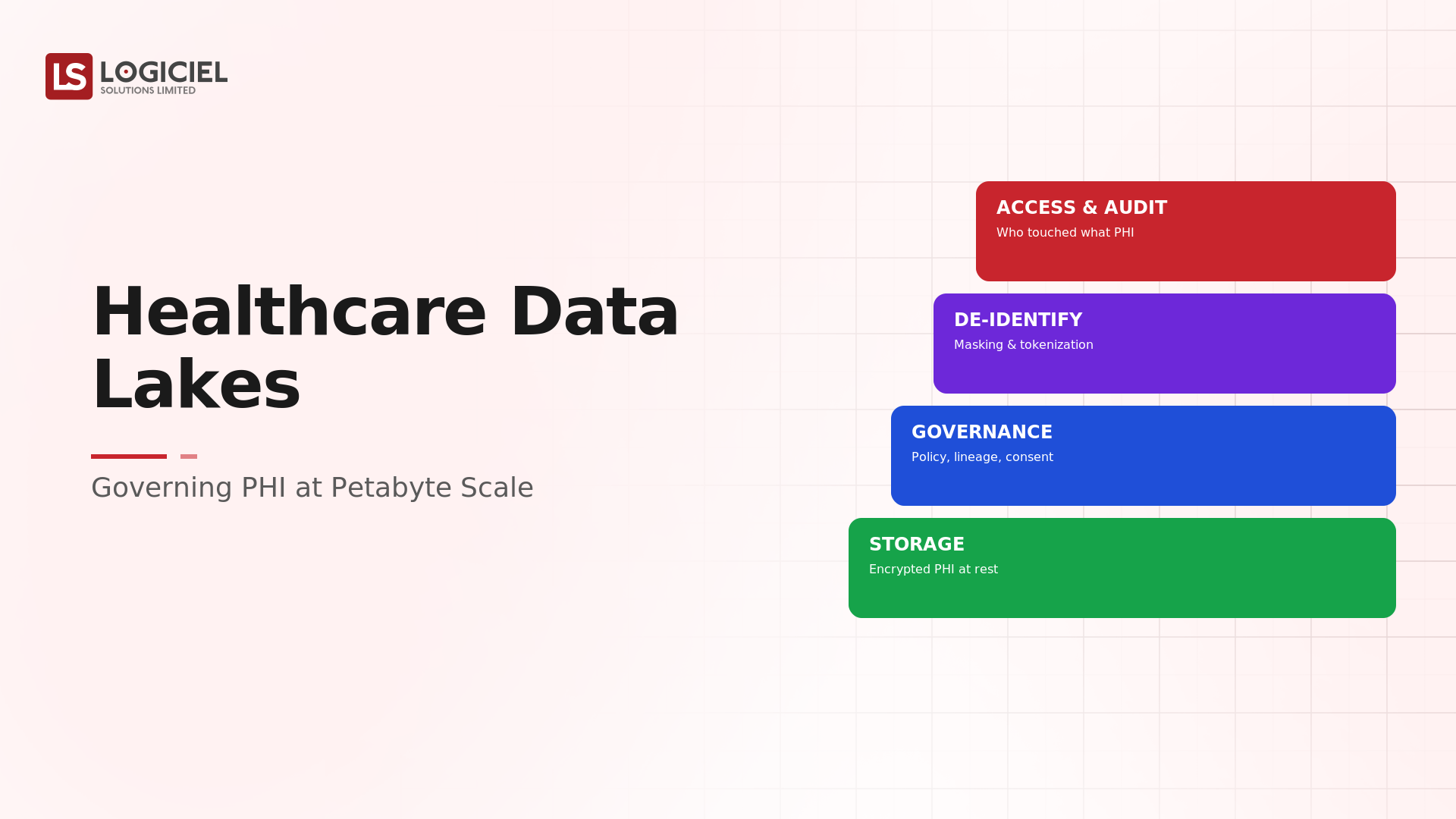
- Healthcare Data Lakes: Governing PHI at Petabyte Scale
At Logiciel Solutions, we work with healthcare architects on FHIR-native design, interoperability, and standards conformance. Our reference patterns come from production healthcare interoperability programs.
Explore how to design a FHIR-native architecture for real interoperability.
Frequently Asked Questions
What is a FHIR-native architecture?
An architecture that uses FHIR resources as the internal data model, stored and exchanged as FHIR, so interoperability is built into the system rather than achieved by translating to FHIR at the boundary. FHIR is what the system is, not just what it speaks to outsiders.
How is FHIR-native different from supporting a FHIR API?
Supporting a FHIR API can be a thin translation over a proprietary core, veneer interoperability that loses nuance and multiplies per-partner mapping. FHIR-native uses FHIR as the actual model throughout, delivering seamless exchange and far lower connection cost.
Why does edge-translation FHIR not scale?
Because a proprietary core forces bespoke mapping for each partner and ripples mappings through every data model change. Translation loses nuance and the work grows with every connection, whereas a FHIR-native core exchanges natively with any FHIR partner.
How do we handle local requirements in FHIR-native design?
With FHIR profiles and extensions that meet local needs within the standard, rather than proprietary divergence that breaks conformance. Combined with terminology services and validation, this keeps the architecture both locally useful and interoperable.
What is the biggest mistake in healthcare interoperability?
Treating FHIR as a format to translate to at the API boundary over a proprietary core, and calling that interoperability. It is a veneer that loses nuance, multiplies mapping work, and does not deliver seamless exchange. Use FHIR as the internal model and stay conformant.