The Initiative That Did Not Reach Patients
A director of population health at a health plan described an analytics initiative to me that her team had launched in 2023. The initiative built a sophisticated risk model identifying patients at high risk of heart failure exacerbation. The model performed well in validation. The team presented results to leadership. The leadership approved the initiative.
Two years later, the model was still operating. The patient outreach that the model was supposed to drive had not happened systematically. Care coordinators received occasional reports. Some patients got outreach when coordinators had capacity. Most did not. The model had identified patients who needed intervention. The intervention had not been delivered at scale.
She told me the experience reflected a pattern she had seen across population health AI initiatives. Analytics succeed. Intervention delivery fails. The gap between knowing who needs help and delivering that help is where most population health AI programs lose value.
The pattern is common. Population health AI investment concentrates on the analytical side because that is where data scientists and engineers spend their time. The intervention delivery side requires operational capacity, organizational coordination, and patient engagement that the analytical work alone does not produce.
The programs that produce outcomes follow recognizable patterns that span both analytics and intervention. Knowing the patterns prevents the gap.
Healthcare Data Standardization
Why clinical AI accuracy degrades when code sets update, how ontology mapping breaks across EHR vendors, and the canonical data layer.
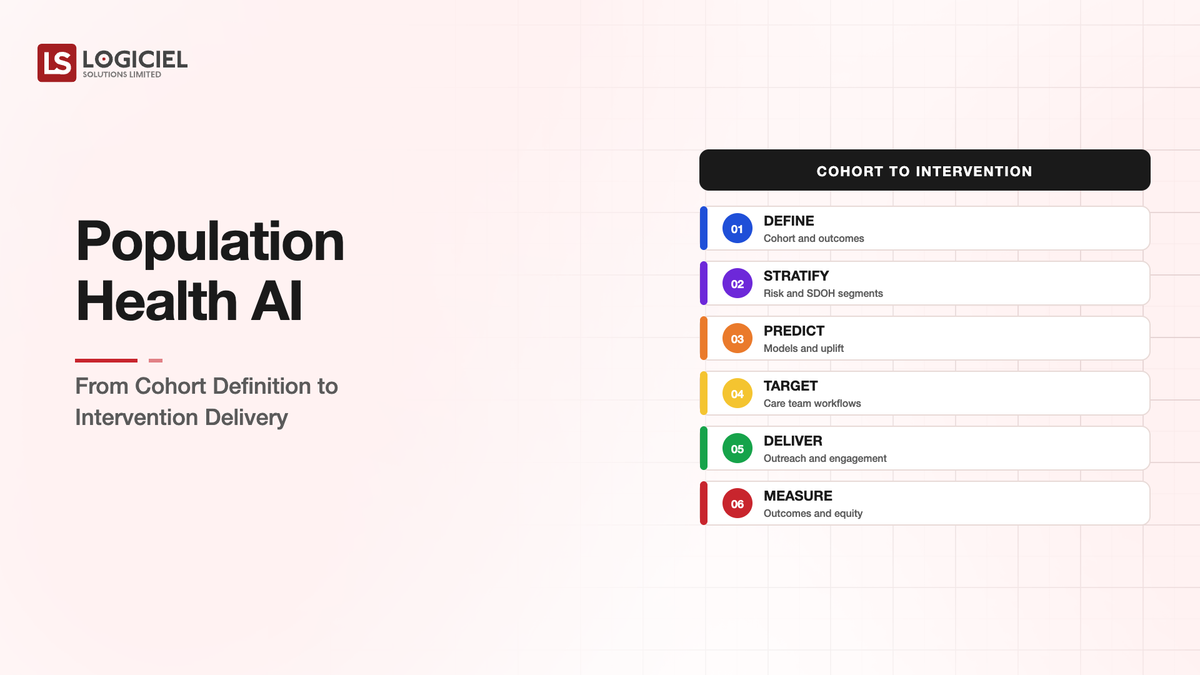
The Four Stages and What Each Has to Deliver
Population health AI work that produces patient outcomes operates across four stages. Each stage has specific deliverables. Programs that under-invest in any stage produce gaps that affect outcomes.
The first stage is cohort definition. The program identifies which patients to focus on. The definition combines clinical criteria, risk factors, and intervention opportunity. A cohort that is too broad cannot be served. A cohort that is too narrow misses patients who would benefit.
The deliverable is a documented cohort definition with clear inclusion and exclusion criteria. The criteria can be expressed as code that produces the actual cohort from current data.
The second stage is risk stratification within the cohort. The program identifies which patients within the cohort have highest priority for intervention. The stratification considers clinical risk, intervention amenability, patient capacity to engage, and resource availability.
The deliverable is a prioritized list with appropriate context. Each patient on the list has documented reasoning for inclusion and priority level.
The third stage is intervention delivery. The program reaches the prioritized patients with appropriate interventions. The interventions are evidence-based and patient-appropriate. The delivery happens at scale.
The deliverable is documented intervention contact with each patient on the prioritized list, with outcome of the contact and follow-up actions.
The fourth stage is outcome measurement. The program measures whether interventions produced the intended outcomes. The measurement informs ongoing program refinement.
The deliverable is outcome data linked back to the intervention activity. The data supports both program evaluation and individual patient care.
Programs that complete all four stages produce outcomes. Programs that stop at stage two (which is what the opening example illustrates) produce analytics that does not translate to patient impact.
What Distinguishes Programs That Reach Stage Four
Programs that successfully execute all four stages share recognizable characteristics.
The first characteristic is operational ownership that spans analytics and delivery. The same leader has accountability for both the analytical work and the intervention delivery. Without unified ownership, the analytical team produces lists and the delivery team handles whatever they can; the gap between them does not close.
The second characteristic is intervention delivery capacity sized for the cohort. The care coordinators, community health workers, pharmacists, or other intervention deliverers exist in numbers that can reach the identified patients. Without sufficient capacity, the program identifies more patients than it can serve.
The third characteristic is patient engagement design that accounts for the patient experience. The intervention is delivered in ways patients can engage with. Cultural appropriateness, language accessibility, communication channel preferences, scheduling flexibility all get attention. Without engagement design, the delivery reaches some patients and misses others systematically.
The fourth characteristic is closed-loop measurement that informs both program operation and individual care. The outcomes feed back to the program for refinement. Individual outcomes feed back to clinical teams caring for specific patients. Without the loop, the program operates without feedback.
These characteristics are organizational and operational rather than primarily technical. The technical work matters; the technical work alone does not produce outcomes.
Where AI Specifically Helps
AI applications in population health span the four stages with specific patterns.
In cohort definition, AI helps identify patients who fit cohort criteria but may not have explicit diagnosis codes. NLP on clinical notes catches conditions documented in narrative. Pattern recognition identifies patients whose clinical patterns match cohort criteria even without explicit categorization.
In risk stratification, AI provides more accurate risk scoring than traditional rule-based approaches. Multivariate models that integrate many risk factors produce better stratification than single-factor approaches. The improvement is measurable across multiple disease cohorts.
In intervention delivery, AI supports personalization at scale. Outreach communications can be customized to patient characteristics. Timing can be optimized for patient engagement patterns. The customization happens at volume that human-only delivery cannot match.
In outcome measurement, AI helps track interventions and outcomes across complex data sources. Linking interventions to outcomes requires combining clinical data, intervention records, claims data, and patient-reported outcomes. AI-assisted analytics handles the complexity better than manual analysis.
These AI applications support but do not replace the operational work that the four stages require.
What Goes Wrong With Population Health AI
Three patterns of program failure recur.
The first pattern is overinvestment in analytics relative to delivery. The team builds sophisticated models and produces prioritized lists. The delivery infrastructure cannot serve the lists. The lists pile up. The analytics impressively predicts outcomes that the program cannot affect.
The second pattern is intervention delivery without good targeting. The team delivers interventions broadly without using analytics to focus. The interventions cost substantial resources and produce diluted impact. The analytics that could have focused the interventions sits unused.
The third pattern is operational handoff that breaks between teams. The analytics team produces lists. The delivery team operates on different priorities. The communication between teams is partial. Patients fall through the gaps.
Each pattern is preventable through unified program ownership and balanced investment across stages.
What This Costs
Population health AI programs that span all four stages typically require substantial investment. The analytics team, the delivery capacity, the patient engagement infrastructure, and the measurement capability all need adequate funding.
For a health plan or health system serving a population of several hundred thousand members, program investment typically lands in the $2M-$10M annual range across analytics and operations. The investment supports specific cohorts with specific interventions.
The return on investment for well-executed programs typically shows up in two to four years. Reduced hospitalizations, improved outcomes, lower total cost of care for the targeted cohorts. The return justifies the investment when the program executes all four stages.
Programs that stop at stage two do not produce return on investment. The analytics cost is real; the outcomes are not.
Ambient Clinical Documentation
The three engineering challenges that determine whether ambient AI documentation ships into a health system or fails security review.
Call to Action
What Logiciel Does Here
Logiciel works with health plan and provider population health teams designing or operating population health AI programs. The work is typically structured around assessment of current stage coverage and architecture appropriate to the specific cohort and intervention design.
The Healthcare AI Implementation framework covers the three risk tiers that population health programs navigate. The Data Pipelines for Real-time Claims Processing framework covers the claims data infrastructure that population health programs depend on.
A 30-minute working session is enough to assess your current population health program against the four-stage model.
Frequently Asked Questions
How do I start a population health AI program?
With a specific cohort where the intervention is well-understood and the delivery capacity exists. Hypertension management. Diabetes care. Heart failure exacerbation prevention. Specific cohorts with established interventions produce faster outcomes than broad programs.
What about social determinants of health?
Increasingly important for population health programs. SDOH data integration with clinical data improves cohort definition and intervention design. The data sources are less mature than clinical data; the patterns are evolving.
How do I measure ROI for population health programs?
Through quasi-experimental designs comparing intervention cohorts to matched non-intervention cohorts. Pure randomized trials are rare in population health; well-designed comparative analyses produce defensible ROI estimates.
What about patient engagement at scale?
Multi-channel engagement with preference-based delivery. Text, phone, secure messaging, mail. Patients have different channel preferences. Programs that match channels to preferences see higher engagement than single-channel programs.
How does this differ from clinical decision support for individual patients?
Population health works at cohort level with focus on intervention efficiency at scale. Clinical decision support works at encounter level with focus on individual patient guidance. The two are complementary; many programs use both. Sources: - CMS, "Population Health Management Strategy 2024-2026" - JAMA Network, "AI in Population Health Management," 2024